

Dave Chase (@chasedave), CEO of Avado, spoke at the Collaborative Health Consortium's weekly Pilots and Collaborations call last Friday.
Dave led with the quote from Dr. Josh Umbehr:
"A good scalpel makes a better surgeon. Good communication makes a better doctor."
Communication (and understanding how information flows) is the critical tool for physicians to get the information they need to make the best choices they've been trained to make.
On the same day, Dr. Jim Yong Kim was named as President Obama's choice as the new head of the World Bank. Just last night I watched an interview that Dr. Kim did in 2009 with Bill Moyers that focuses largely on health care. During the interview, Dr. Kim talked about Southwest Airlines and how what they're thinking might do for medicine:
"they have taken seriously the human science of how you transfer simple information from one person to the next...What we need now is a whole new cadre of people who understand the science, who really are committed to patient care. But then also think about how to make those human systems work effectively. We've been calling it, aspirationally, the science of health care delivery."
Dr. Kim is talking about many things here, social networks, health care experience design, network science and in other parts of the interview he talks about the need for reducing variability with such thing as Kiazen or Lean. It's risk reduction in care delivery through continuous feedback, learning and understanding information flows in networks of people, systems and care delivery processes.
Patient engagement means helping patients (and their physicians) make better decisions
It struck me that Dr. Kim and Dave Chase are talking about something very similar, if not the same thing: networks, communication flows and decision-making.
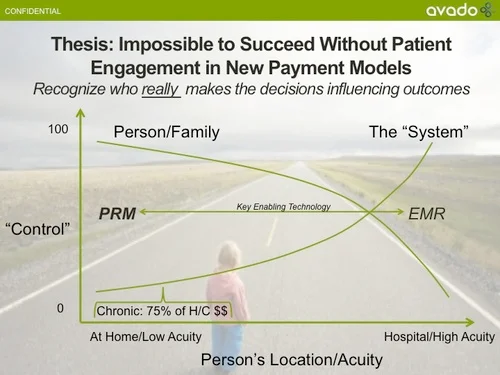
Dave Chase talked about the need for patient engagement and "control" in this brilliant slide from Avado:
You can see the rest of the slides Dave has given us permission to post here (great presentation).
When we talk about patient engagement and control, we're largely talking about who has control over decision making, how to engage them, and how to help influence that decision-making through information with flows and feedback.
In the graph above to the left in the "At Home/Low Acuity" area, this is where ACOs and new payment models' success or failure will be determined. As Dave notes, this is ultimately 75% of health care costs that are behavioral, based on decisions that patients and families make day in and day out. Understanding behavior networks in health care is critical. Fowler and Christakis' Connected that does a deep dive into how behavior patterns transfer through real social networks (not just the online variety).
While Dr. Kim and the Dartmouth school of Care Delivery are focused on the right side of the graph, in a patient's accute phase when they are in the clinic or in the hosptial, but the realization is the same:
We need to understand what engages people, what information is needed and when to help patients and their care team make the right decision and reduce the risk of a bad outcome.
It's Network Science for health care.
Network Science in health care
The fledgling field of Network Science has been studied and applied in fields such as UX design, big data (scaled learning) CRM systems (be sure to read Michael Wu, @mich8elwu,'s posts on this), social network analysis, lean (and lean startups), Kaizen, open source, open innovation and supply chain logistics, and yes, Moneyball and now ACOs. It's a network perspective to systemic learning, with accelerated, scaleable learning as the critical measure of success. It's a matter of understanding connections, decisions, engagmement and human factors, information flows and how they all fit together all enabled through feedback. It's the new dialectic.
(For more on this subject, along with Connnected, I highly recommend The Information by Gleick, Thinking, Fast and Slow, by Kahneman, Where Good Ideas Come From by Steven Johnson, and the collected writings of Clay Shirky and John Hagel III to pursue this subject further.)
The Moneyball approach to baseball is a network and systems approach where statistics and critical measures, such as on-base-percentage, or how to approach a specific batter in a specific situation are found to matter more than nuance physical or mental characteristics of the players.
Payment reform, at long last aligning incentives of patient, physician and insurer, we hope, can only be successful with a continuous learning and statistics driven approach similar to what Moneyball did for baseball. Network science and big data are the science of figuring out what works on a large scale. Once systems are connected and health information is digitized, both through payment reform and initiatives such as Stage II meaningful use, we'll be able to make better decisions in medicine. As long as everyone is covered, that's a good thing. It means insureres will focus on keeping well rather than restricting coverage on those who need it most. It a networked world, it means personal responsibility and universal coverage, something both conservatives and liberals could love!
We need people and systems that understand network science in health care
Dr. Kim is right, we need a whole new cadre of people who understand netowrks in health care. This is the science of reducing risk through the understanding of how information moves with various types of networks. We need people who understand the fledgling field of network science in health care. Network Science is the key to driving innovation while reducing costs because it is ultimately about accelerating organizational and systemic learning. New payment models need to find out what works in health care and fast, and both Dr. Kim and Dave Chase understand that what's happeing is that networks of organizations, people, care delivery and technologies can lead to better care and reduced risks -- if we understand how they work.
Looking at network effects and information transfer across a wide variety of disciplines, we are rapidly gaining new insights into risk reduction from a network perspective.
Network science, the science of care delivery, patient engagement, social network analysis, customer/patient relationship management, user experience design, big data, and the algorithms being used now in baseball, are all part of a whole new way of looking at risk and probabilites across a wide variety of disciplines. In medical school and hospitals, as Dr. Kim pointed out, we currently do it ad hoc. For better outcomes, we need to understand these information flows better, so we can learn what works.
ACOs will need to understand very well Jim Yong Kim's research on variation, Dave Chase's work at Avado and even Moneyball. Scaleable learning is rapidly becoming the new basis of competion, even in health care. It's the rocket science of health care.
Next up: Why we need decision-support in health care (Hint: we're all really bad at intuitive statistics)
Read more on Leonard's blog:
- Ideas Are Cheap ...Until they're shared




Comments are closed.